

Product Overview
NAD+ Injection is a compounded prescription formulation of nicotinamide adenine dinucleotide (NAD+), a coenzyme found in all living cells and crucial for fundamental biological processes. NAD+ helps drive cellular energy production by shuttling electrons in metabolic pathways like glycolysis and the Krebs cycle, ultimately enabling ATP synthesis for cell function. Beyond its metabolic role, NAD+ also participates in DNA repair and cell signaling, making it essential for maintaining cellular health and viability.[¹] Natural NAD+ levels decline progressively with age; by middle age, tissues may contain roughly half the NAD+ they had in youth. This age-related NAD+ depletion has prompted interest in NAD+ supplementation strategies to support cellular metabolism and possibly counteract aspects of aging.[²]
Clinically, NAD+ Injection has been explored for a range of potential wellness benefits, although robust evidence in humans remains limited. Advocates propose that boosting NAD+ could increase energy levels, enhance mitochondrial function, and improve fatigue or cognitive clarity in some individuals. NAD+ therapy is also being investigated in contexts like healthy aging and neuroprotection, and it has been trialed as an adjunct in addiction recovery programs to reduce withdrawal symptoms, though formal clinical trial data are still sparse. Importantly, NAD+ Injection is not an FDA-approved drug; it is prepared by licensed 503A compounding pharmaciesand 503B outsourcing facilities for patient-specific and office use with a doctor’s prescription. All potential benefits therefore must be weighed cautiously, and treatment is undertaken under medical supervision given that safety and efficacy are not yet established by regulatory authorities.[³]
NAD+ Injection is supplied by compounding pharmacies as a lyophilized (freeze-dried) sterile powder, typically in vials containing 500 mg or 1,000 mg of NAD+ per vial. The powder is reconstituted with sterile diluent (such as bacteriostatic water) before use to yield an injectable solution. Dosing regimens are individualized, as there is no one-size-fits-all dosage for NAD+ therapy. For general wellness or anti-aging purposes, providers often start with relatively low doses and adjust based on patient response. A common protocol, for example, is to begin with about 20 mg of NAD+ administered subcutaneously and gradually increase the dose over subsequent injections up to around 100 mg per injection. These injections may be given a few times per week; a usual schedule is 1 to 3 times weekly, depending on how well the patient tolerates NAD+ and the goals of therapy¹⁰. By ramping up the dosage slowly, patients can often avoid side effects like headache or nausea while still obtaining the energizing or cognitive benefits of NAD+. A maintenance plan might involve ongoing injections of 50-100 mg weekly or as directed by the prescribing provider. Importantly, NAD+ injections can be administered either in a clinic or self-administered at home if the patient has been properly instructed; the subcutaneous shots are given into the fatty tissue (for instance, the back of the arm or the abdomen) using a small insulin-type syringe for convenience.[¹⁰]
In clinical research settings and certain intensive protocols (such as addiction detoxification), much higher NAD+ dosages have been utilized. For example, one early protocol for substance uses disorders employed 500-1,000 mg of NAD+ per day delivered by slow intravenous infusion over several consecutive days. In that setting, patients received high-dose NAD+ daily for about 4-10 days to alleviate acute withdrawal symptoms, followed by tapering to less frequent booster injections over the ensuing weeks.[⁷] Such large doses are administered under direct medical supervision and via IV drip to ensure safety. Outside of specialized cases, most wellness protocols do not use daily high-dose NAD+; instead, they favor moderate doses spread out over time. Ultimately, the dosage and frequency of NAD+ Injection must be tailored to the individual’s needs, tolerability, and treatment objectives. A healthcare provider will determine the appropriate starting dose and titration schedule for each patient. They will also set an upper limit on the total weekly dose (for example, some experts recommend not exceeding ~300 mg per week in subcutaneous dosing without further evaluation) to minimize any risk of adverse effects.[¹³] As with any compounded therapy, ongoing monitoring is part of dosage management; the provider may adjust the dose based on the patient’s energy levels, symptom improvements, or any side effects. Through this personalized approach, NAD+ Injection dosing can range from small booster doses to larger infusions, but always under professional guidance to ensure it remains safe and effective for the patient’s condition.[¹³]
NAD+ plays a central role in cellular energy metabolism and is required for the proper function of mitochondria. In its oxidized (NAD+) and reduced (NADH) forms, this coenzyme cycles between metabolic reactions, accepting and donating electrons during nutrient breakdown and ATP generation. Each stage of respiration, from glycolysis in the cytoplasm to the citric acid cycle and oxidative phosphorylation in mitochondria, depends on NAD+/NADH to carry reducing equivalents, thereby driving the production of cellular energy⁴. By supplying additional NAD+ to the body, NAD+ Injection may help ensure these energy-producing pathways can proceed optimally, particularly in situations of NAD+ depletion. In addition, NAD+ serves as a substrate for numerous enzyme systems that regulate cell function. For example, NAD+-dependent enzymes include the sirtuins (SIRT1-7), a family of protein deacetylases involved in gene expression, stress responses, and metabolic regulation, as well as poly(ADP-ribose) polymerases (PARPs) that assist in DNA repair. Sufficient NAD+ availability is necessary for these enzymes to operate, so raising NAD+ levels could in theory modulate pathways related to aging, inflammation, and cell survival.[⁵]
While the precise mechanisms of action for NAD+ therapy’s purported benefits are not fully elucidated, multiple lines of research suggest several contributing effects.[⁶] NAD+ augmentation may counteract age-related NAD+ loss caused by overactive NAD-consuming enzymes (such as the NADase CD38), thereby supporting mitochondrial maintenance and metabolic homeostasis. Laboratory studies in cell and animal models of accelerated aging have shown that replenishing NAD+ can restore mitochondrial function and stimulate beneficial cellular recycling processes like mitophagy. It is postulated that through these mechanisms, NAD+ repletion might improve cellular energy capacity and resistance to oxidative stress. However, in human systems the outcome of boosting NAD+ is complex and likely involves numerous pathways, from enhanced activity of sirtuins (implicated in longevity and metabolic control) to improved DNA damage repair, all of which are areas of ongoing investigation⁵. In summary, NAD+ Injection provides additional coenzyme substrate that may broadly support the cell’s energy-producing and regulatory enzymes, but its exact biological effects in people remain an area of active research and may vary depending on individual physiology.[⁶]
At present, NAD+ Injection has no well-defined absolute contraindications aside from hypersensitivity to NAD+ or any ingredient in the formulation. Individuals with a known allergy to NAD+ or its preparation components must avoid this therapy. Because NAD+ is a form of vitamin B3-related compound, true allergic reactions are uncommon; however, any prior adverse reaction to niacinamide/NAD+ products would warrant against use of NAD+ Injection. There are no other officially reported contraindications specific to NAD+ as of now, but the absence of documented contraindications largely reflects limited clinical study; it does not guarantee that NAD+ therapy is appropriate for everyone⁷. Physicians therefore evaluate each patient’s health status before recommending NAD+ injections and exercise caution in certain scenarios even in the absence of formal contraindication labels.
In practice, providers may advise against NAD+ injections in patients with serious underlying medical conditions as a precaution. For example, those with severe liver or kidney impairment, unstable heart disease, or other significant systemic illnesses are typically approached carefully if considering NAD+ therapy. The metabolism and elimination of NAD+ (and its by-products) could be altered in advanced hepatic or renal dysfunction, and high-dose NAD+ might theoretically affect cardiovascular dynamics, so practitioners generally avoid or closely supervise NAD+ use in such settings. Similarly, individuals with active cancer are usually counseled not to use NAD+ Injection. NAD+ supports fundamental energy pathways in all cells, including cancer cells, raising concern that artificially boosting NAD+ might fuel malignancy growth or interfere with certain cancer treatments. Although a direct causal link between NAD+ supplementation and cancer progression has not been proven, experts recommend that patients with an ongoing cancer or a history of cancer only consider NAD+ therapy with clearance from their oncologist⁹. In summary, while NAD+ Injection is a broadly applicable metabolic therapy, it should not be used by anyone allergic to it, and it is generally avoided in pregnant women, cancer patients, or those with serious chronic diseases, absent compelling medical rationale. All candidates for NAD+ therapy should be screened by a qualified provider to ensure no individualized contraindications or safety concerns.[⁸]
No significant drug-drug interactions with NAD+ Injection have been identified in the medical literature to date. NAD+ is a form of a naturally occurring coenzyme/vitamin, and it does not appear to directly interfere with common medications or supplements based on current knowledge. In clinical use thus far, patients receiving NAD+ infusions or injections have not shown notable interaction effects with other drugs; for instance, there are no reports of NAD+ altering the metabolism of prescription medications or diminishing their efficacy. However, the absence of known interactions may partly reflect the limited scope of formal studies on NAD+ therapy, so this lack of interactions should be interpreted with caution. It remains possible that as NAD+ use becomes more widespread, some interactions could emerge. For this reason, patients are advised to inform their healthcare provider of all medications, supplements, or herbs they are taking before starting NAD+ injections, even though no incompatibilities are documented thus far.[¹²] Healthcare providers will monitor any unusual responses and can adjust treatment if any potential interaction is suspected.
One practical consideration during NAD+ Injection therapy is the management of NAD+ metabolism by-products. When NAD+ is administered, it is ultimately metabolized to nicotinamide (vitamin B3) as it is utilized in the body. Excess nicotinamide is eliminated partly through a methylation pathway, meaning it consumes methyl donors in the process of excretion. To support this metabolic process, some clinicians recommend co-supplementation with a methyl donor such as trimethylglycine (TMG) while on NAD+ injections¹⁰. TMG can help replenish methyl groups and facilitate the clearance of nicotinamide, theoretically reducing the buildup of by-products that could cause fatigue or headaches in some individuals. Though this is not an interaction in the traditional sense, it is an adjunctive measure that may improve tolerance of NAD+ therapy. Aside from such supportive strategies, patients do not typically need to avoid any specific foods, drinks, or medications while on NAD+ Injection. Nevertheless, it is prudent to have regular medical supervision, so any subtle interaction or side effects can be promptly identified and managed appropriately. Overall, NAD+ Injection is considered compatible with most other therapies, with no known adverse drug interactions, but comprehensive disclosure of one’s medication regimen to the treating provider is important for safe care.[¹²]
NAD+ Injection is generally reported to be well-tolerated, with a low incidence of serious adverse effects. Because NAD+ is a molecule naturally present in the body, the administration of pharmaceutical NAD+ tends to produce only mild, transient side effects in most people. Common reactions can include fatigue, nausea, headache, or lightheadedness during or after an injection. Some individuals experience a sensation of warmth, flushing, or slight dizziness, especially if the infusion or injection is given rapidly. There may also be minor irritation at the injection site, for example, redness, tenderness, or a brief burning sensation where the NAD+ solution is injected subcutaneously. These localized reactions typically resolve quickly. Gastrointestinal upset is infrequent but has been noted (e.g. a few patients have reported stomach discomfort or loose stools).[⁸] Overall, these side effects are short-lived and manageable, often improving by slowing the rate of administration or taking breaks during an intravenous infusion if needed.
Crucially, the side effect profile of NAD+ largely depends on dosage and infusion rate. Early case reports suggested that delivering NAD+ too rapidly can provoke acute symptoms. For instance, in one 1960s study of intravenous NAD+ for addiction, patients who received a fast IV drip experienced immediate headache and shortness of breath, whereas those given the same dose at a slower drip rate (under ~35 drops/min) had no distress⁷. To minimize such effects, clinics now administer NAD+ infusions slowly (over several hours) or use divided subcutaneous doses. If patients do experience headaches, chest tightness, or dizziness during an NAD+ infusion, it is often relieved by pausing or slowing the infusion rate. Other reported side effects have been mild muscle fatigue or feeling “chilled” during a long infusion, which likewise tend to subside afterward. In rare instances, high-dose NAD+ might transiently elevate markers of liver function (such as bilirubin or enzyme levels), but these changes have not been clinically significant and normalize shortly after treatment.[¹¹]
Notably, clinical studies to date have not identified any severe or lasting adverse events attributable to NAD+ Injection. In a pilot trial of NAD+ intravenous infusion in healthy adults, subjects receiving 750 mg of NAD+ over 6 hours reported no negative symptoms at all, and there were no vital sign abnormalities or serious laboratory derangements compared to placebo.[¹¹] This reinforces that NAD+ therapy, when administered in a controlled medical setting, has a favorable safety profile. Still, because NAD+ injections are a relatively novel therapy, patients are monitored for any unexpected reactions. Allergic reactions to NAD+ are extremely rare, but as with any injectable substance, there is a remote possibility of hypersensitivity; signs like rash, itching, or swelling would necessitate immediate medical attention. Additionally, standard injection risks (infection at injection site, vein irritation for IV, etc.) apply, though proper sterile technique makes these complications uncommon.[⁸] Overall, NAD+ Injection’s side effects are mild and manageable, and serious side effects appear rare. Patients often finish NAD+ treatment reporting positive effects (such as increased energy or mental clarity) with few downsides aside from the transient discomforts noted above. Nevertheless, ongoing surveillance and research are important to fully characterize long-term safety as use of this therapy expands.
The safety of NAD+ Injection has not been established in pregnancy, and its use is not recommended for pregnant women. NAD+ has critical roles in fetal development and maternal metabolism, but there is a lack of any controlled data on administering high-dose NAD+ to pregnant patients. Because no studies have evaluated potential risks, such as effects on the fetus or pregnancy outcomes, clinicians advise against NAD+ therapy during pregnancy out of an abundance of caution.
Similarly, women who are breastfeeding should avoid NAD+ injections, since it is unknown whether the exogenous NAD+ could affect the nursing infant or alter milk composition. Until more information is available, NAD+ Injection is only initiated in non-pregnant adults, and women of childbearing potential are typically asked about pregnancy status before starting therapy. If a patient becomes pregnant while receiving NAD+, the treatment would be discontinued unless there were extraordinary circumstances and a careful risk-benefit assessment by the healthcare provider. In summary, due to insufficient safety data, NAD+ Injection is contraindicated in pregnancy and during breastfeeding to protect both mother and child⁷. All potential female patients are screened and counseled on this point, and effective contraception is recommended for those undergoing NAD+ therapy if applicable.
Proper storage of NAD+ Injection is important to maintain its stability and potency. Pharmacies typically ship NAD+ as a dry lyophilized powder, which should be kept at controlled room temperature (approximately 20°C to 25°C / 68°F to 77°F), protected from excessive heat, moisture, and light. Until it is reconstituted, the powder vial should be stored in its original container, tightly sealed and away from any humid environments (to prevent degradation). Once the NAD+ powder is mixed with diluent to create the injectable solution, the unused solution must be kept refrigerated at 2°C to 8°C (36°F to 46°F).[⁷] The reconstituted NAD+ is not preserved for long periods at room temperature, so refrigeration is necessary to slow any breakdown of the product. Patients receiving multi-dose vials are instructed to store the vial in the fridge between uses. Additionally, compounded NAD+ solutions come with a beyond-use date (BUD) after which any remaining solution should be discarded; this is often around 90 days from compounding when refrigerated, or shorter if stored at room temperature as stability permits. Once a vial has been punctured and is in use, it is generally recommended to discard any leftover solution after ~28 days for sterility reasons (even if within the chemical BUD). NAD+ Injection should be always kept out of reach of children and pets. When disposing of any unused NAD+ solution or expired vials, one should follow proper medical waste protocols: do not pour it down drains or flush it. Instead, discard through a pharmacy take-back program or as instructed by the healthcare provider or pharmacist. By adhering to these storage guidelines, patients can ensure that each dose of NAD+ Injection remains effective and safe up until its indicated expiration.
- Johnson, S., & Imai, S. I. (2018). NAD+ biosynthesis, aging, and disease. F1000Research, 7, 132. https://doi.org/10.12688/f1000research.12120.1
- Massudi, H., Grant, R., Braidy, N., Guest, J., Farnsworth, B., & Guillemin, G. J. (2012). Age-associated changes in oxidative stress and NAD+ metabolism in human tissue. PLoS ONE, 7(7), e42357. https://doi.org/10.1371/journal.pone.0042357
- Braidy, N., Villalva, M. D., & van Eeden, S. (2020). Sobriety and satiety: Is NAD+ the answer? Antioxidants, 9(5), 425. https://doi.org/10.3390/antiox9050425
- Cantó, C., Menzies, K. J., & Auwerx, J. (2015). NAD+ metabolism and the control of energy homeostasis: A balancing act between mitochondria and the nucleus. Cell Metabolism, 22(1), 31-53. https://doi.org/10.1016/j.cmet.2015.05.023
- Belenky, P., Bogan, K. L., & Brenner, C. (2007). NAD+ metabolism in health and disease. Trends in Biochemical Sciences, 32(1), 12-19. https://doi.org/10.1016/j.tibs.2006.11.006
- Fang, E. F., Hou, Y., Lautrup, S., et al. (2019). NAD+ augmentation restores mitophagy and limits accelerated aging in Werner syndrome. Nature Communications, 10(1), 5284. https://doi.org/10.1038/s41467-019-13172-8
- Conlon NJ. The Role of NAD+ in Regenerative Medicine. Plast Reconstr Surg. 2022 Oct 1;150(4 Suppl ):41S-48S. doi: 10.1097/PRS.0000000000009673. Epub 2021 Sep 28. https://pmc.ncbi.nlm.nih.gov/articles/PMC9512238/
- Superpower. (n.d.). Informed medical consent: NAD+ injections. Superpower.com. Retrieved June 11, 2025, from https://superpower.com/informed-medical-consent/nad-injections
- Palmer, R. D. (2021). Nicotinamide adenine dinucleotide and the sirtuins caution: Pro-cancer functions. Aging Medicine, 4(4), 337-344. https://doi.org/10.1002/agm2.12184
- AgelessRx. (n.d.). NAD+ Injection - FAQs. Agelessrx.com. Retrieved June 11, 2025, from https://agelessrx.com/faq/
- Grant, R., Berg, J., Mestayer, R., et al. (2019). A pilot study investigating changes in the human plasma and urine NAD+ metabolome during a 6-hour intravenous infusion of NAD+. Frontiers in Aging Neuroscience, 11, 257. https://doi.org/10.3389/fnagi.2019.00257
- Alam, K. (2025, March 31). NAD+ (Nicotinamide adenine dinucleotide): Benefits, usage, and safety information. Hone Health. Retrieved June 11, 2025, from https://help.honehealth.com/hc/en-us/articles/7867064833303
- Invigor Medical. (2023). NAD+ FAQs. Invigor Medical Help Center. Retrieved June 11, 2025, from https://help.invigormedical.com/en/articles/7016924-nad-faq-s
- Swiss Medica. (n.d.). NAD+ Therapy - benefits and dosages. SwissMedicaUSA.com. Retrieved June 11, 2025, from https://swissmedicausa.com/nad-therapy
- Avellina Aesthetics. (n.d.). NAD+ injection in Philadelphia. Avellinaaesthetics.com. Retrieved June 11, 2025, from https://www.avellinaaesthetics.com/philadelphia-nad-plus-injection/
What is NAD+ Injection?
NAD+ Injection is a compounded injectable medication containing nicotinamide adenine dinucleotide (NAD+), a vital coenzyme that supports cellular energy production and DNA repair. By delivering NAD+ directly into the body, these injections aim to increase NAD+ levels beyond what might be achieved with oral supplements or diet¹. It’s essentially a way to replenish a naturally occurring molecule that tends to decline with age, under the guidance of a healthcare provider.
How does NAD+ Injection work in the body?
NAD+ Injection works by providing additional NAD+ for the body’s cells to be used in metabolic and regulatory processes. NAD+ is crucial as a coenzyme in reactions that generate ATP (energy) in cells, and it also serves as a substrate for enzymes involved in DNA repair and gene regulation. When administered, NAD+ can be absorbed into tissues (or converted into precursor forms that enter cells) and may enhance the efficiency of mitochondrial energy metabolism. The exact mechanisms are complex, but broadly NAD+ injections may counteract NAD+ depletion and support better cellular function, especially in high-demand tissues like the brain and muscles.[⁴]
What are the potential benefits or uses of NAD+ injections?
NAD+ injections are used in integrative and functional medicine settings for a variety of potential benefits, although research is still emerging. Patients and providers have reported anecdotal improvements in energy levels, reduced fatigue, and enhanced mental clarity or focus following NAD+ therapy. NAD+’s role in cellular repair has also made it a popular experimental therapy for improved health in aging, with the idea that maintaining higher NAD+ might support healthy aging processes. Some addiction recovery programs utilize NAD+ infusions to potentially help alleviate withdrawal symptoms and cravings, as NAD+ is thought to aid brain-cell recovery in substance use disorders³. Additionally, NAD+ has been investigated for improving metabolic health, possibly benefiting conditions like metabolic syndrome by supporting better insulin sensitivity and mitochondrial function. It’s important to note that these uses are considered off-label and exploratory; individuals may experience positive outcomes, but large-scale clinical evidence is limited. Results can vary, and NAD+ injection is usually one component of a broader wellness or treatment plan.[³]
What side effects can NAD+ Injection cause?
Most people tolerate NAD+ injections well, but some side effects can occur. Common mild side effects include headache, nausea, dizziness or lightheadedness, and sometimes a sensation of warmth or flushing during the injection⁸. Some patients report feeling fatigued or having mild brain fog shortly after a dose, which usually resolves quickly. There can also be minor irritation at the injection site, such as redness or soreness. These effects are generally transient and ease as the rate of injection is slowed, or the body adjusts. Serious side effects are rare; there have been no reports of organ damage or severe reactions directly linked to NAD+ in clinical studies¹¹. However, any time you receive an injection, there’s a very small risk of infection or allergic reaction; if you experienced swelling of the face, rash, or difficulty breathing (signs of a possible allergy), you would need immediate medical attention. Overall, NAD+ Injection side effects tend to be manageable, and your provider will monitor you, especially during initial doses, to ensure you’re responding well.
Who should not use NAD+ Injection?
NAD+ injections are not for everyone. You should not use NAD+ if you have a known allergy to NAD+ or any ingredient in the injection; although this is uncommon, any history of hypersensitivity to niacinamide or NAD would be a contraindication. Additionally, individuals with active cancer are generally advised against NAD+ therapy due to theoretical risks of fueling cancer cell metabolism⁹. It’s also prudent to be cautious or avoid NAD+ injections if you have a serious uncontrolled medical condition (for example, end-stage liver or kidney disease or severe heart disease), unless your physician specifically determines it’s safe. And as discussed below, NAD+ is not recommended for women who are pregnant or breastfeeding. Always discuss your full medical history with the prescribing doctor; they will determine if NAD+ Injection is appropriate or if any conditions you have would preclude its use.
Can NAD+ injections be used during pregnancy or breastfeeding?
No, NAD+ Injection is not recommended for pregnant or breastfeeding women⁷. The effects of high-dose NAD+ on a developing fetus or nursing infant have not been studied, so the therapy is avoided entirely in these situations out of caution. If you are pregnant or planning to become pregnant, you should not start NAD+ injections. Likewise, mothers who are breastfeeding are advised against NAD+ therapy because it’s unknown if or how NAD+ might pass into breast milk and affect the baby. The consensus among providers is to wait unless more safety data becomes available. Always inform your healthcare provider if you become pregnant while on NAD+ therapy; they will likely discontinue the injections to err on the side of safety.
Do NAD+ injections interact with any medications or supplements?
There are no known drug interactions with NAD+ Injection currently.[¹²] NAD+ doesn’t appear to adversely interact with common medications; for instance, it’s not known to affect how other drugs are metabolized or to block their action. That said, absence of known interactions doesn’t guarantee that none exist. It’s always important to tell your healthcare provider about all other medicines or supplements you are taking so they can monitor for any unusual effects.[¹²] So far, NAD+ therapy has been used alongside standard treatments (like antidepressants, for example) without incident. Additionally, because NAD+ supports metabolic pathways, some practitioners recommend taking a methyl donor supplement (such as TMG, trimethylglycine) concurrently, to aid in processing any excess nicotinamide produced; this is more of a supportive measure than an interaction concern. In summary, you can generally continue your other medications while on NAD+ injections, but keep your medical team informed and always follow their advice if they prefer to adjust dosing schedules or monitor certain lab parameters.
How is NAD+ Injection given to patients?
NAD+ can be administered in a couple of ways, depending on the dose and setting. Intravenous (IV) infusions are one method; NAD+ is diluted in IV fluid and slowly dripped into a vein over several hours, typically done in a clinic. This is often used for high-dose therapy or acute treatment (such as in some addiction programs). For lower maintenance doses, NAD+ is frequently given as a subcutaneous injection, meaning a small volume is injected just under the skin (for example, in the abdomen, thigh, or back of the arm).[¹⁰] Subcutaneous injections are relatively quick (done in a few minutes) and can be administered in a doctor’s office or self-administered at home if the patient is comfortable with it. In either case, the healthcare provider will provide detailed instructions. The subcutaneous route has the advantage of a slow release into the bloodstream and is quite convenient for ongoing therapy. Some protocols might also use intramuscular injections (into muscle), though subcutaneous is more common due to better tolerability. The important thing is that NAD+ must be given by injection or infusion to be effective; taking NAD+ by mouth is not effective since NAD+ is not absorbed intact. Your provider will choose the administration route that matches your treatment plan and teach you how to properly give the injections if you’ll be doing them at home.
What is the typical dosage and frequency of NAD+ injections?
Dosage can vary widely. For general wellness or anti-aging purposes, many protocols use about 50-100 mg of NAD+ per injection, given a few times per week.[¹³] A common approach is starting on the lower end (e.g. 50 mg) and working up to 100 mg per dose if tolerated, with injections perhaps 2-3 times weekly. Some patients might then continue with weekly injections at 100 mg as maintenance. In more intensive therapy scenarios (such as for chronic fatigue or recovery support), a practitioner might recommend a series of daily injections over 5-10 days at 100-250 mg per day, then taper to a maintenance schedule. The maximum dose in a single day or infusion is usually around 500-1,000 mg in clinical research settings.[⁷] That high dose is reserved for special cases and always done under medical supervision (generally via slow IV infusion). For home use injections, providers often advise not exceeding a cumulative ~300 mg per week unless there’s a specific indication.[¹³] Your exact dosage and frequency will be personalized; the doctor considers factors like your age, symptoms, and treatment goals. They will monitor how you feel and may adjust the plan accordingly. NAD+ isn’t a one-size-fits-all therapy, so it might take some trial to find the optimal dosing schedule for your needs. Always follow the protocol your healthcare provider sets, and don’t increase the dose or frequency on your own, to ensure safety and best results.
Do I need a prescription for NAD+ Injection and is it FDA-approved?
Yes, NAD+ Injection requires a prescription from a licensed healthcare provider. It is a compounded medication made by specialized pharmacies, so you can only obtain it legally with a doctor’s prescription through a 503A compounding pharmacy. NAD+ injections are not FDA-approved.[¹⁵] ; meaning the Food and Drug Administration has not evaluated or authorized this formulation for any specific medical condition. The therapy is used off-label based on emerging science and clinical experience. Because it’s not FDA-approved, insurance may not cover it, and the quality is ensured through the compounding pharmacy’s standards rather than an FDA drug approval. That said, reputable compounding pharmacies operate under strict regulations, and your provider works with them to get a high-quality NAD+ product. The lack of FDA approval also means that definitive safety and efficacy trials are still forthcoming. If you’re considering NAD+ therapy, make sure you do so under the guidance of a knowledgeable physician who can obtain it via prescription and monitor your treatment appropriately. Never purchase NAD+ injections directly online without a prescription; not only is it illegal, but product quality and sterility would be uncertain. With a proper prescription, you’ll receive NAD+ from a regulated pharmacy along with instructions for safe use.[¹⁵] Always feel free to discuss with your provider why NAD+ is recommended in your case and what the current evidence is, since it is a newer therapy outside of standard FDA-approved treatments.
Disclaimer: This compounded medication is prepared under section 503A of the U.S. Federal Food, Drug, and Cosmetic Act. Safety and efficacy for this formulation have not been evaluated by the FDA. Therapy should be initiated and monitored only by qualified healthcare professionals.
Administration Instructions
Intramuscular Injection Instructions
Reconstitution Instructions
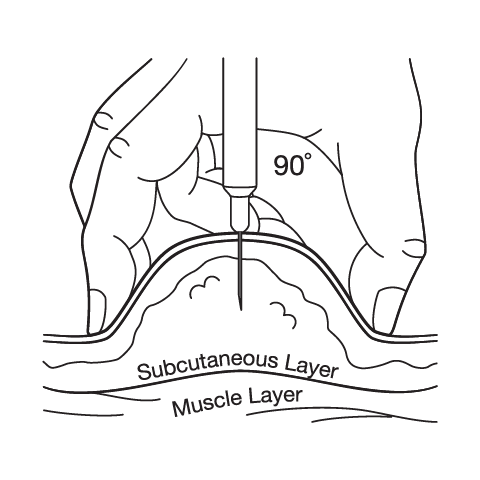
Subcutaneous Injection Instructions
Related medications
 NAD+ Injection (Aqueous)
NAD+ Injection (Aqueous) NAD+ Cream
NAD+ Cream NAD+ Nasal Spray
NAD+ Nasal Spray Cyanocobalamin (Vitamin B12) Injection
Cyanocobalamin (Vitamin B12) Injection Tirzepatide / Niacinamide Injection
Tirzepatide / Niacinamide Injection Methylcobalamin Injection (Vitamin B12)
Methylcobalamin Injection (Vitamin B12) Sermorelin Acetate Injection
Sermorelin Acetate Injection Testosterone Cypionate Injection
Testosterone Cypionate Injection Anastrozole Capsules
Anastrozole Capsules Enclomiphene Citrate Capsules
Enclomiphene Citrate Capsules Vitamin B-Complex Injection
Vitamin B-Complex Injection503A vs 503B
- 503A pharmacies compound products for specific patients whose prescriptions are sent by their healthcare provider.
- 503B outsourcing facilities compound products on a larger scale (bulk amounts) for healthcare providers to have on hand and administer to patients in their offices.
Frequently asked questions
Our team of experts has the answers you're looking for.
A clinical pharmacist cannot recommend a specific doctor. Because we are licensed in all 50 states*, we can accept prescriptions from many licensed prescribers if the prescription is written within their scope of practice and with a valid patient-practitioner relationship.
*Licensing is subject to change.
Each injectable IV product will have the osmolarity listed on the label located on the vial.

Given the vastness and uniqueness of individualized compounded formulations, it is impossible to list every potential compound we offer. To inquire if we currently carry or can compound your prescription, please fill out the form located on our Contact page or call us at (877) 562-8577.
We source all our medications and active pharmaceutical ingredients from FDA-registered suppliers and manufacturers.